Specialists Shun People of Color
July 27, 2021
Racial and Ethnic Disparities in Outpatient Visit Rates Across 29 Specialties.
JAMA Internal Medicine Online First
July 19, 2021
By Christopher Cai et al.
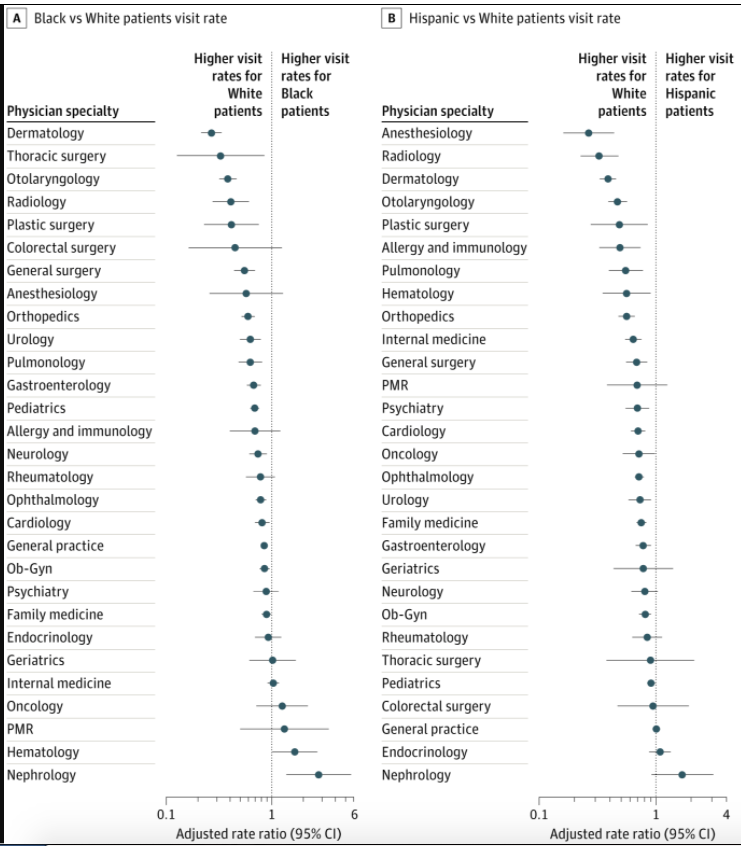
[Using nationally representative data from the Medical Expenditure Panel Survey] We tabulated office and outpatient department visits to each physician specialty and calculated adjusted rate ratios (ARRs) for each racial/ethnic minority group (compared with the White population).
Black individuals had low visit rates (vs White individuals) to most specialties (23 of 29 [79.3%]. Among specialties with many visits, Black:White disparities were particularly marked for dermatology (ARR 0.27; 95% CI, 0.21-0.34), otolaryngology (0.38; 95% CI, 0.32-0.46), plastic surgery (0.41; 95% CI, 0.23-0.75), general surgery (0.55; 95% CI, 0.44-0.69), orthopedics (0.59; 95% CI, 0.51-0.69), urology (0.62; 95% CI, 0.50-0.78), and pulmonology (0.63; 95% CI, 0.48-0.81). Black individuals had higher visit rates to nephrologists (2.78; 95% CI, 1.37-5.62) and hematologists (1.65; 95% CI, 1.0-2.70) and similar visit rates to internists, geriatricians, and oncologists.
For Hispanic and Asian/Pacific Islander individuals, visit ratios (compared with White individuals) were … significantly lower for 20 of 29 (69.0%) and 21 of 27 specialties (74.1%), respectively. Similar patterns were present for Native American individuals, although the 95% CIs were wide.
The study findings demonstrate a consistent pattern of racial and ethnic disparities in outpatient care, implicating systemic defects that are best characterized as structural racism.
Figure (partial, to fit):
Comment by David Himmelstein and Steffie Woolhandler
This study (disclosure: we’re co-authors) provides yet more evidence of the pervasive effects of white supremacy in medical care. Black, Hispanic, Asian and Native American people get far less care from virtually every medical and surgical specialty than non-Hispanic White individuals.
The inferior insurance coverage (and hence reimbursement to physicians) of Black, Hispanic and Native Americans probably drives much of the disparities for those groups, but people of color had somewhat lower visit rates even after controlling for insurance coverage.
Fixing these inequities in care will require erasing financial distinctions among patients by assuring that everyone’s insurance pays the same fees, and that co-payments and deductibles are banned. Only a comprehensive single payer reform can achieve that. But additional measures will also be needed: e.g. greatly increasing the ranks of minority physicians; offering grants to practices to locate in minority neighborhoods; and changing the racist culture that permeates many medical institutions.
You might also be interested in...
Recent and Related Posts
Political Party Split vs Concurrence on Government Guarantee of Health Care
Cross-National Insurance Contrasts in Amusing 1-minute Videos