Medicare REACH: Financial Incentives will Undermine Doctor-Patient Trust
July 16, 2022
Summary: Hidden in the fine print of the REACH program launched by CMS to transform traditional fee-for-service Medicare we discover a pivotal, nasty feature: Physicians will share in the financial savings achieved by capitated contractors. This destroys more than 50 years of beneficiary confidence that doctors’ decisions are based on their best medical interests.
ACO Realizing Equity, Access, and Community Health (REACH) Model Request for Applications
Centers for Medicare & Medicaid Services (CMS)
February 24, 2022
All Participant Providers and Preferred Providers … may receive a distribution from the ACO of any shared savings payment received by the ACO …
ACO REACH Model PY2023 Participant and Preferred Provider Management Guide
Centers for Medicare & Medicaid Services (CMS)
Revised June 2022
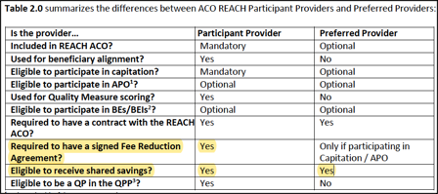
Comparing GPDC to the ACO REACH Model
CMS
February 2022
A very detailed table, to explain REACH to the public. However, NO mention of sharing savings with providers.
Comment by: Jim Kahn
I’ve focused on various problems that will plague REACH, most recently the leeway permitted for fast diagnostic upcoding and thus rapid profit growth.
Then, the worst feature of all, hiding in the program details, jolted me: REACH is structured to make doctors complicit in the money game. Specifically, they can receive a portion of the “shared savings” generated when their patients use fewer Medicare resources than the capitation amount. With a discount imposed on their regular fees, the pressure to reduce care and thus recoup income is immense.
To be crystal clear: when doctors reduce or delay care, by skipping diagnostic tests or referrals to specialists or treatments, and their patients spend less overall, doctors get a financial bonus by receiving a portion of the savings.
And when doctors participate in diagnostic upcoding, they share in the resulting increased savings under the higher capitation level.
With REACH contractors permitted to keep ALL of the first 25% in savings, the incentive to reduce care is powerful. And with doctors eligible to receive a slice of those savings, clinical decisions will have two competing masters: patient well-being and provider income.
So, for nearly six decades, traditional Medicare beneficiaries could count on doctors to focus on their well-being, with no incentive to save (or, with the early ACOs, a very small incentive).
This central program feature is spelled out in contractor documents (request for proposal, program guidance), but not mentioned in the CMS material disseminated to the public. I think I know why: CMS knew it would be hugely unpopular.
We need to save traditional Medicare, by ending REACH and removing for-profit intermediaries and the co-opting of physicians. We need to focus on patient welfare. We need single payer!
You might also be interested in...
Recent and Related Posts
Hobbling Health & Human Services