US Mortality High & Strongly Linked to Wealth
A new cross-national study highlights two stark facts: Mortality is substantially higher in the US than in counterpart European nations, and it is more closely associated with wealth stratum (inversely, of course). Health insurance and wealth inequality play central roles.
April 26, 2025
Association between Wealth and Mortality in the United States and Europe
New England Journal of Medicine
April 2, 2025
By Sara Machado et al
In the United States, there has been a massive transfer of wealth from the middle class to the wealthy in the past 60 years, which has increased wealth inequality. Other high-income countries have seen concurrent growth in wealth inequality, but these have been less pronounced than in the United States. Life expectancy in the United States is also lower than in other high-income countries, and it is decreasing. These are of key concern, particularly because increases in mortality are most pronounced among the poorest people.
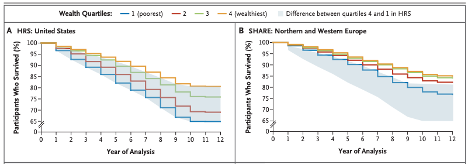
[Interpretation: Survival over time among adults 50-85 years old is lower in the US than in Northern / Western Europe, with more spread by wealth level.]
From the Discussion
We found that wealth was associated with mortality across the United States and Europe and that the difference in mortality between the top and bottom quartiles of wealth appeared to be larger in the United States than in Europe. Mortality in the United States was higher than in Europe, even at higher wealth levels.
Comment by: Don McCanne & Jim Kahn
We have reported often that the US can greatly increase the access and affordability of health care by enacting and implementing a well-designed, single payer, improved version of Medicare that is provided to all.
However, as this study indicates, our health is also broadly linked with economic disparities. The well recognized problem of wealth inequality in the US is associated with reduced life expectancy, especially afflicting lower-wealth individuals, far more than in European nations. At the same time, when compared to those nations – with comprehensive universal health care systems – all US wealth levels have higher mortality, even at the top tier. So the wealthy should understand that they will gain life expectancy if the system is fixed overall. Single payer is not about trade-offs, it’s about improvements for everyone.
What does this tell us? Clearly, as we have said for decades, our nation’s overall health would improve with an improved system of Medicare for All. But it also demonstrates that we need a more equitable distribution of wealth which would be more likely if we also had an equitable system of income distribution. The study showed that life expectancy was related to wealth. However, it is very difficult to see how wealth could be made more equitable without ensuring adequate income for everyone. We also really need a progressive wealth tax if we are going to correct the profound inequities created by today’s preoccupation with the accumulation of mega-wealth.
This is not the same as calling for equal income and wealth. Instead, it is a plea for fairness and justice in income and wealth distribution instead of the creation of centi-billionaires made possible by denying middle- and lower-income workers their fair share of society’s productivity. This, of course, requires effective government oversight, unlike the inhumane, slash-and-burn administration we have today.
What can we do? In just 100 days, extensive damage has been initiated to our socioeconomic and legal systems, and much more is threatened. So reversing the current politics and policy is an emergency. Once we have control of the situation, we can move forward with changes that will let us function like our European friends, perhaps even better. Solving our major challenges would enhance our nation’s well-being and return us to a place of leadership and admiration in the world. Our progress will increase global well-being! But it’s up to the people to act.
About the Commentator, Jim Kahn
Jim (James G.) Kahn, MD, MPH (editor) is an Emeritus Professor of Health Policy, Epidemiology, and Global Health at the University of California, San Francisco. His work focuses on the cost and effectiveness of prevention and treatment interventions in low and middle income countries, and on single payer economics in the U.S. He has studied, advocated, and educated on single payer since the 1994 campaign for Prop 186 in California, including two years as chair of Physicians for a National Health Program California.
See All PostsYou might also be interested in...
Recent and Related Posts
Public Provisioning of Services: Adjunct to Single Payer